
Anatomy
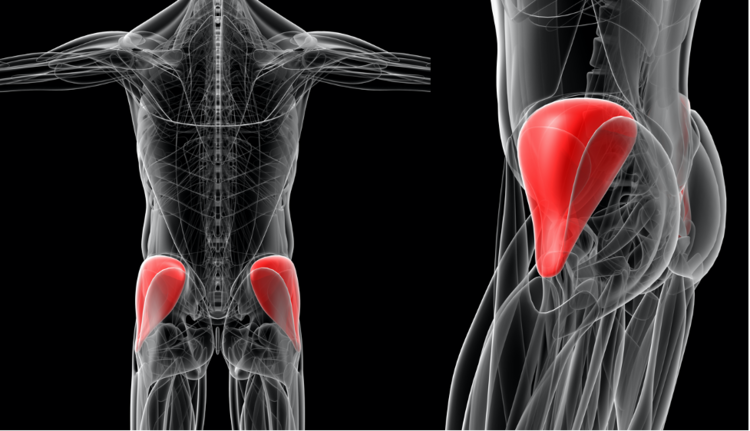
The gluteus medius and minimus are adjacent muscles in the hip area that are responsible for hip abduction (taking the leg away from the midline) as well as stabilizing hip rotation motion (internal rotation). They also assist with hip flexion. Above all, they are the primary hip abductors.
The gluteus medius muscle attaches at the superior lateral portion of the iliac crest of the pelvis and lies superficially over the gluteus minimus, and underneath portions of the gluteus maximus (posteriorly) and the tensor fascia lata (anteriorly). The distal attachment is at the lateral facet of the greater trochanter of the femur bone.
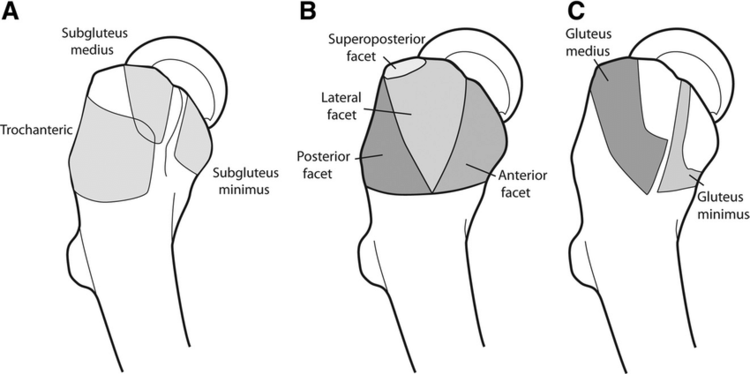
The gluteus minimus muscle attaches at the external surface of the ilium, lying inferior to the gluteus medius muscle. The distal attachment is located at the anterior facet of the greater trochanter.
The gluteus medius and minimus help with our normal activities of walking, running, standing, and climbing stairs.
Etiology
Gluteal tendon tears are fairly common, affecting about 25% of late to middle-aged women and 10% of middle-aged men.
Gluteal tendon tears can occur for several reasons:
Degenerative Tearing
-
Chronic peritrochanteric (lateral hip) disease (i.e., IT band friction, prolonged weakness, tendinopathy)
-
Systemic disease
-
Vascular disease
Acute Trauma
-
Falls
-
Blunt trauma
Overuse
Diagnosis
Gluteal tendon tears are diagnosed using a full history and physical examination, which likely includes testing such as X-rays and Magnetic Resonance Imaging (MRI).
Gluteus medius and minimus tears typically reveal themselves with lateral-sided hip pain that can begin with or without traumatic injury. Weakness is also a common complaint, which gradually decreases and may cause other symptoms in and around the hip joint and pelvis. Changes in walking patterns are also frequent. Pain is often aggravated with walking, running, standing for longer periods of time, rising from seated positions, and going up or down stairs.
To confirm this diagnosis, if suspected, advanced imaging is required to confirm the location and extent of the tendon injury. This helps to guide a comprehensive, focused treatment program.

MRI of the pelvis illustrating a full-thickness tear of the left gluteus medius tendon with retraction of the tendon.
Treatment
Gluteus medius and minimus tears are graded based on how extensive the injury is. Low-grade to high-grade partial thickness tears may be treated conservatively with various methods. Full-thickness tears will likely not heal adequately to regain full strength and function. Treatment options are approached with the entire person in mind, as there may be multiple factors that make treatment more likely to be beneficial vs potentially harmful.
Conservative Care Options:
-
Oral medications – Non-steroidal anti-inflammatory medications (NSAIDs)
-
Activity modifications – avoidance of stressing the gluteal tendon tear by avoiding stairs, aggravating exercise and motions are key.
-
Injections
-
Steroid injections may offer temporary relief of pain in an effort to improve the conditioning of the hip’s supporting musculature and soft tissues.
-
Biologics injections: PRP (platelet-rich plasma) or BMAC (Bone Marrow Aspirate Concentrate) is also an option that allows for the body’s natural healing cells to provide pain relief and optimize a healing environment for the injury.
-
-
Physical therapy: Through multiple methods of addressing the body’s current condition, physical therapy can strengthen the surrounding musculature, stretch excessively tight soft tissues, and also optimize the healing environment for the injured tissue.
Surgical Care Options:
-
Endoscopic repair of gluteus medius and/or minimus tendon: Utilizing arthroscopic techniques, the injured tendon can be repaired to its anatomic position, utilizing anchors with sutures to securely affix the tendon.
-
Open repair of the gluteus medius and/or minimus tendon: For full-thickness tears that have retracted, an open technique may be required to provide full visualization and access to the injured tendon to complete an anatomic repair, securing the tendon utilizing suture anchors.
-
These techniques may be combined with other hip procedures in the same setting depending on other conditions that may need to be treated in the same setting.
Dr. Dold specializes in the management of all hip conditions, including the management, both surgical and non-surgical, of gluteus medius and minimus tears. To schedule a new patient consultation, please fill out a form and a member of our team will reach out to you within 24 hours to confirm your appointment.
Sources:
Acute Traumatic Tear of the Gluteus Medius and Gluteus Minimus in a Marathon Runner
Prevalence of abductor mechanism tears of the hips in patients with osteoarthritis.
Acute Traumatic Tear of the Gluteus Medius and Gluteus Minimus in a Marathon Runner