
Definition
To understand hip dysplasia, we first need to understand the anatomy of the hip joint. The hip is a ball and socket joint located at the pelvis, with the acetabulum making the “socket” side of the joint, and the head of the femur, making up the “ball” side of the joint.
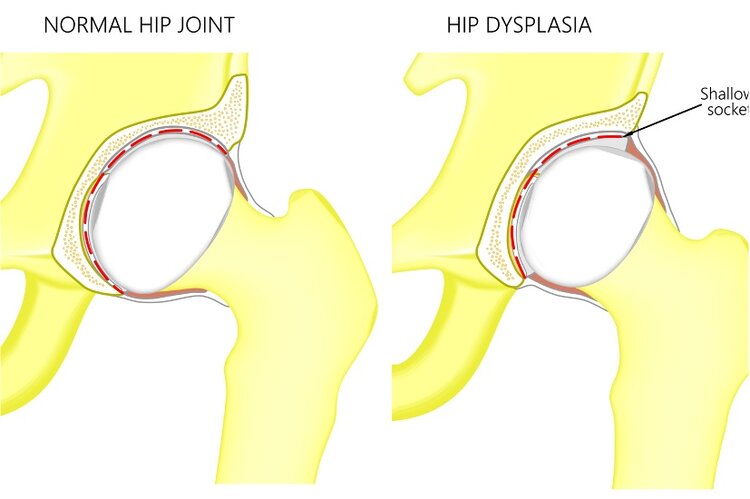
Although there is no single clinical definition of hip dysplasia, the main characteristic of hip dysplasia is an underdevelopment of the socket portion, or acetabulum, of the hip joint. This may be present in one or both hips of an individual.
Etiology
Hip dysplasia is thought to originate due to multiple factors around the time of childbirth and early developmental years. Factors that may precipitate the development of congenital hip dysplasia include fetal position during gestation in the womb, as well as positioning during infant years. Risks during infancy for developing dysplasia include children being placed in a neutral hip position (no hip flexion) either with swaddling or with child carriers. Genetic disposition is another factor in hip dysplasia, meaning if there is a family history of hip dysplasia, it may be more likely passed down through generations.
As children develop, there is a natural growth of the acetabulum to cover the head of the femur, leading to “normal” anatomy. In dysplasia, the acetabulum never fully covers the head of the femur. This may lead to a host of symptoms and complications.

Diagnosis
Hip dysplasia is mainly a radiographic diagnosis, meaning that it is diagnosed based off of parameters and measurements found on plain x-rays of the pelvis and hips. However, hip dysplasia may show itself prior to any symptoms with subluxation or dislocation of the hip as early as childbirth.
In skeletally mature patients, symptoms may first be noticed as anterior, lateral or posterior hip pain, or feelings of instability as well as limping. As time passes, hip dysplasia may lead to acetabular labral tearing and early onset osteoarthritis. Not only can issues at the hip be experienced, but spine and lower extremity issues may also be present from attempts to correct this malalignment through modifications.
Treatment
Hip Dysplasia is treated differently throughout the lifespan. During infancy, hip dysplasia with or without subluxation or dislocation is most often treated with bracing which allows the developing hip to have the adequate contact to stimulate bone growth and appropriate coverage of the femoral head.
As the skeleton matures, there are multiple treatment options available to help to decrease symptoms and improve function for those with hip dysplasia.
Conservative care options:
Oral medications – Non-steroidal anti-inflammatory medications
– Activity modifications – abducted (wide stance) position for weight bearing activity may improve symptoms by changing alignment to a more ‘normal’ anatomic position.
– Injections – Steroid injections may offer temporary relief of pain in an effort to improve conditioning of the hip’s supporting musculature and soft tissues.
Surgical Care options:
-
Periacetabular Osteotomy, or PAO – This is a procedure that aims to correct the alignment of the acetabulum to provide the adequate coverage of the femoral head in order to decrease symptoms.
-
Hip Arthroscopy – For those that sustain acetabular labral tears due to hip dysplasia, hip arthroscopy may be a necessary procedure after the alignment of the hip is corrected. This procedure is not indicated in first line treatment of hip dysplasia.
-
Total hip arthroplasty – 20-40% of those suffering with osteoarthritis of the hip develop this condition due to hip dysplasia. This procedure not only provides treatment for the arthritis that has developed, but with careful planning, can also help to improve alignment of the hip joint.
Dr. Andrew Dold specializes in both hip arthroscopy and hip arthroplasty (hip replacement) surgery. For a new patient consultation, please submit a form with your information and a team member will contact you within 24 hours.
Review Article:
Hip Dysplasia in the Young Adult